Model-Informed Drug Development in Drug Discovery
It’s well known that developing a new drug or therapeutic is resource intensive. Much of the cost and time spent goes toward seemingly promising projects that end in late-stage clinical failures. Applying modeling and simulation, or model-informed drug discovery and development (MID3) approaches early in R&D helps build confidence and understanding within a project before significant resources have been allotted. For example, modeling and simulation approaches can help teams determine how reasonable or difficult it will be to develop a therapeutic and whether the optimal parameters are favorable. The goal is to ultimately identify the “failures” early-on and accelerate and optimize the “winners” to the clinic.
Early Feasibility Assessment
Early feasibility assessment (EFA) is the application of validated, pharmacologically relevant systems pharmacology models to help predict whether a therapeutic has a reasonable chance of success. Traditionally, the developability of a therapeutic has been estimated using best guesses, back-of-the-envelope calculations, general rules of thumb, or empirically. Given the increase in complexity of therapeutics, especially biologics such as bispecific antibodies, tri- or multi-specific antibodies, antibody drug conjugates (ADCs), conditionally active antibodies, gene therapies, and T cell engagers, these non-MID3 approaches become risky as there are many factors that can impact feasibility, and many are not straightforward or intuitive. EFA is a systematic, quantitative, methodical MID3 approach that can help project teams in early discovery determine whether a therapeutic enters the portfolio, what experiments are most important moving forward, or hypotheses early on in a project. Following is a list of common applications or questions where EFA has assisted project teams.
- Which step(s) of the signaling cascade should we consider targeting?
- What are potentially optimal drug properties?
- What affinities may we need (e.g. 1 pM vs. 1 nM) given a desired coverage?
- What parameters may I need to attain a reasonable therapeutic index?
- Selectivity (e.g. 10x, 100x, 1000x) for desired target to improve therapeutic index or to reduce sink effects?
- Helps with ‘Which of our preclinical candidates should we move forward?’
- Will targeted-mediated drug disposition (TMDD) potentially be an issue? If so, can it be reduced?
- How do I prioritize my experiments?
- How do I optimize my experimental design in the context of study limitations?
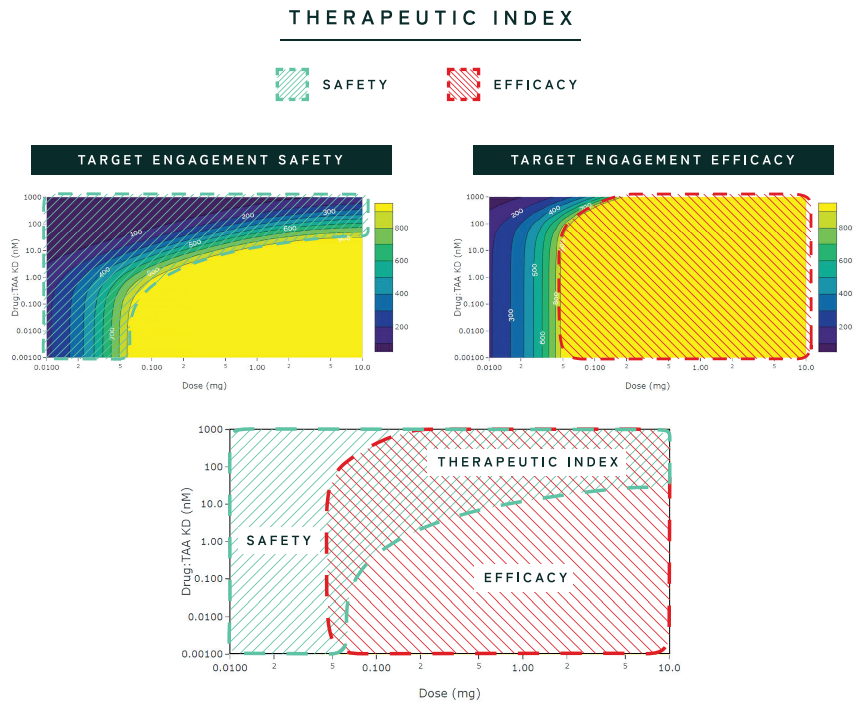
Determining Therapeutic Index
Therapeutic index (TI) is the range of doses at which a drug or therapeutic is effective without unacceptable adverse events. This can be thought of as finding the sweet spot where a therapeutic is efficacious but still safe. Determining TI is very challenging, especially for complex biologics, gene therapies, and cell therapies, but it is critical to calculate early on to determine if the therapeutic is worth investing in, even before internal data is generated.
MID3 enables project teams to scan across various drug parameters, dose ranges, and biological parameters to determine if a TI exists. For example, in the case of a T cell engager (TCE) bispecific biologic, a math model enables you to predict the peak amount of trimer formed and binding to tumor cells versus on target, off-target cells in a variety of different dose or parameter scenarios. This helps you determine if there is a window, or TI, where there is a minimum amount of binding as a surrogate for efficacy where there is also minimum binding to off-target cells which represents safety. The advantage of this computational approach is that numerous simulations are performed in a shorter amount of time than if analyzed via the lab or in animal studies, leading teams to clearer hypotheses and insight into the likelihood that a TI exists and what experiments should follow to confirm this.
Therapeutic R&D Software
Applied BioMath Assess™* is an interactive, web-based application that helps assess the difficulties and risks in developing a therapeutic very early-on using pre-built models and a point-and-click interface. Pre-built models are available for a variety of common pharmacologies, including monospecific and bispecific therapeutics with or without avidity and cell engagers. Other pharmacology models will be released in the near future. In addition, companies may customize their model and/or their analysis with Applied BioMath’s modeling team.
Learn about Applied BioMath Assess
*Patent pending
Early Feasibility Assessment Example
Challenge: A team wants to design a bispecific antibody. All of the targets are cell membrane bound. Their primary, or anchor, target is known and they’re considering five different secondary targets. They need the ability to cover multiple target antigens with a format that has a fixed stoichiometry at a competitive dose and regimen. On paper, when linked with the anchor target, the five secondary targets looked equally efficacious, but they only had resources to support one or two bispecific programs. How can they use MID3 to identify which one or two bispecific antibody pairs they should move forward with?
How MID3 Helped: In this scenario, EFA helped to guide the design of the bispecific antibody by estimating what affinity was required to obtain the desired target engagement/inhibitor, the optimal format with respect to half-life, and the optimal valency with respect to target coverage and avidity. The analysis helped identify the two projects that were 1) the easiest to develop (e.g., affinity, avidity, half-life, TMDD), with the easiest dose regimens (amount, frequency) for the largest simulated patient group (number of cells, sites per cell), 2) the fewest number of sensitive model parameters and uncertainty (which may be understood as meaning fewer experiments), and 3) more confidence in literature values (again, meaning fewer experiments and confidence in predictions). The MID3 analyses would be complemented with in vitro/in vivo experiments.