Background
Determining the feasibility of a biotherapeutic early-on in a project is important and challenging. There’s often no experimental data, not a lot of resources and budget, and many teams resort to back-of-the-envelope calculations or general rules of thumb. Once the project does enter the portfolio, the race is on. It's critical to have a good understanding as early as possible of what therapeutic parameters are necessary to meet the required dosing regimen and success criteria, even theoretical, and also if therapeutic properties (in the form of mathematical model parameters) are feasible (e.g., affinity, half-life, and format). Applied BioMath AssessTM was developed to provide an interactive, web-based tool to help more easily and quickly determine the risk of developability of a therapeutic given a target profile (e.g., indication, desired dose amount and frequency, therapeutic mechanism of action and target coverage or inhibition) and biological parameters (e.g., ligand expression, ligand turnover, receptor per cell, receptor turnover, ligand-receptor affinity, etc.).
In this case study, we explore some of the analyses possible in Applied BioMath Assess using a single compartment, anti-ligand model as an example. Our goal is to determine an acceptable binding affinity and first order half life given prerequisites such as dosing route and frequency for an anti-TNF monoclonal antibody under consideration for patients with rheumatoid arthritis who are on methotrexate. We have simplified this analysis for illustrative purposes. For example, we will assume that the joint, or disease compartment, is well perfused, so we will combine the joint compartment with the central compartment, and use a one-compartment version of the model. We will also assume that there is no soluble receptor and that the concentration of receptor in the blood compartment is 0.1 nM. The mechanism of action for the therapeutic is an antagonist, with an assumed success criteria target inhibition of >95% ligand - receptor inhibition for the entire dosing interval.
-
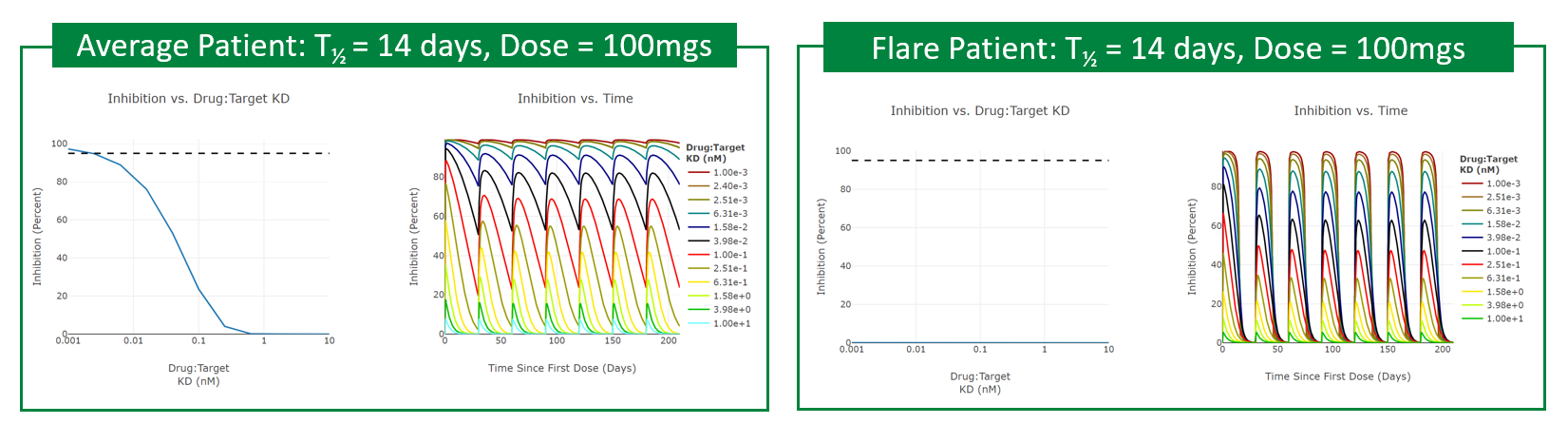
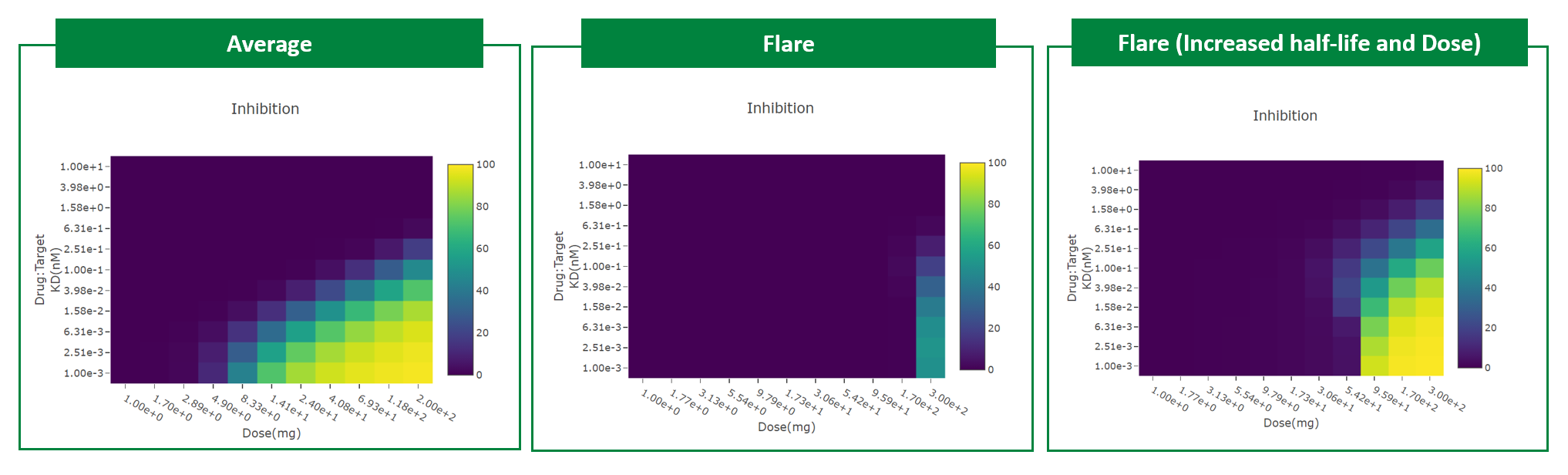
Our analysis shows that for an average patient (0.005 nm) or high expressing case (0.05 nM), a binding affinity of about 2.5 pM or tighter, given a half-life of 14 days, will achieve the success criteria of >95% ligand - receptor inhibition.
-
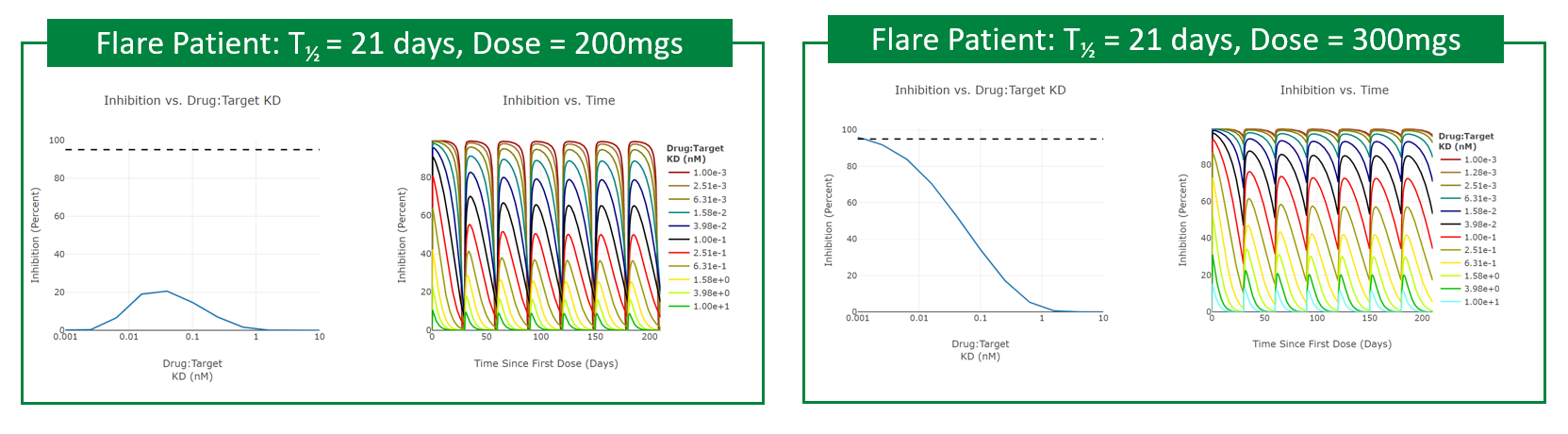
For flare situations, there is no reasonable binding affinity that achieves the success criteria given the dosing regimen, half-life, and solubility. However, if you extend the therapeutic’s first-order half-life to 21 days and increase solubility to 300 mgs, or apply two SC doses at 150mg per SC stick, then a 1pM binder will suffice. Additionally, if you change from monthly SC dosing to every other week, a dose of 150mgs and a 4pM binder will suffice.